First a definition:
Disease: disease is a particular abnormal condition, a disorder of a structure or function that affects part or all of an organism. It may be caused by factors originally from an external source, such as infectious disease, or it may be caused by internal dysfunctions, such as autoimmune diseases. Diseases usually affect people not only physically, but also emotionally, as contracting and living with a disease can alter one’s perspective on life, and one’s personality.
In our every day lives we do not often consider dental disease to be the same as Medical diseases. This is false. In fact dental diseases are the most common diseases that affect people.
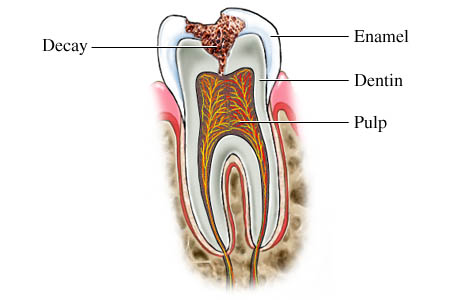
Decay
Dental decay or caries (caries is Latin for “rottenness), also known as cavities, is a breakdown of teeth due to acids produced by bacteria that live on and around the teeth. In a sense, teeth are essentially a form of limestone. If you have ever put an acid like vinegar or lemon juice on limestone the solution will bubble and fize. This action is the result of the acids eating away the calcium/phosphate structure of the rock. The same happens to teeth.
Where do acids come from?
Regarding decay, the acids come from the bacteria in the mouth fermenting residual sugars left over in your mouth after you eat. This fermentation produces acids that are held close to the tooth surface. The more sugar you eat and the more frequently you eat or drink the more opportunity the bacteria have to produce acids.
They are what you eat…Not all bacteria are equal.
The bacterial in your mouth is past on to you by your parents as is most of the bacteria that live on and around you. If you routinely eat a diet that has a high amount of refined carbohydrates the bacterial will shift to include more of the most efficient fermenters, which equals more acids and higher risk for decay. If you limit simple sugars in your diet the bacteria will shift away from this group. This is one reason why two people with equally poor oral hygiene can have very different decay rates.
Dietary and stomach acids can play a role in amplifying the effects of bacterial action. Just as acids produced by bacteria, acids in foods and drink also dissolve and weaken tooth structure. Most often damage from these agents affects the smooth surfaces of teeth. Bacterial activity affects the grooves and other surfaces where bacteria can hide.
Teeth are bathed in saliva and have a coating of bacteria on them (biofilm) that continually forms, almost from the moment they are cleaned. The minerals in the hard tissues of the teeth (enamel, dentin and cementum) are constantly undergoing processes of demineralization and remineralisation. Dental caries results when the demineralization rate is faster than the remineralisation and there is net mineral loss. This happens when there is an ecologic shift within the dental biofilm, from a balanced population of micro-organisms to a population that produce acids and can survive in an acid environment.[5] This shift to a cariogenic microbiological population (one which causes caries) is driven by (eaten) sugars. So, bacteria break down the hard tissues of the teeth (enamel, dentin and cementum) by making acid from food debris or sugar on the tooth surface.[6] Simple sugars in food are these bacteria’s primary energy source and thus a diet high in simple sugar is a risk factor.[6] Risk factors include conditions that result in less saliva such as: diabetes mellitus, Sjogren’s syndrome and some medications.[6] Medications that decrease saliva production include antihistamines and antidepressants among others.[6] Caries are also associated with poverty, poor cleaning of the mouth, and receding gums resulting in exposure of the roots of the teeth.[2][7]
Prevention includes: regular cleaning of the teeth, a diet low in sugar and small amounts of fluoride.[4][6] Brushing the teeth two times per day and flossing between the teeth once a day is recommended by many.[2][6] Fluoride may be from water, salt or toothpaste among other sources.[4] Treating a mother’s dental caries may decrease the risk in her children by decreasing the numbers of certain bacteria.[6] Screening can result in earlier detection.[2] Depending on the extent of destruction, various treatments can be used to restore the tooth to proper function or the tooth may be removed.[2] There is no known method to grow back large amounts of tooth.[8] The availability of treatment is often poor in the developing world.[4] Paracetamol (acetaminophen) or ibuprofen may be taken for pain.[2]
Worldwide, approximately 2.43 billion people (36% of the population) have dental caries in their permanent teeth.[9] The World Health Organizations estimates that nearly all adults have dental caries at some point in time.[4] In baby teeth it affects about 620 million people or 9% of the population.[9] They have become more common in both children and adults in recent years.[10] The disease is most common in the developed world and less common in the developing world due to greater simple sugar consumption.[2]